Anastasia Markiw Builds a New Model for Hospital Lighting
For over a decade, I have been the lighting designer for dozens of plays, musicals, and dance shows. Lighting design has always fascinated me, especially the way lighting can infuse a space with an added layer of emotion. With or without our knowledge, the cycles of our days and the fluctuations of our emotions are dictated by light. Whether experiencing a performance at a theatre, being fatigued at work due to poor lighting conditions, or purposely stumbling in the dark to avoid turning on the bathroom light, everyone has experienced how light impacts daily life.
I started at DesignGroup as a Project Architect in the Healthcare Practice Group in 2017, and, with urging from senior leadership, I decided to finish a second master degree in Healthcare Design at Kent State University. The subject of my year-long thesis was a no-brainer – to combine my two passions by focusing on lighting design in the healthcare setting.
Why Should We Care?
The healthcare industry in the United States accounts for over 16% of the nation’s gross domestic product, and 9% of the energy used in commercial buildings (U.S Department of Energy, 2016). More than 40% of the electricity use in healthcare facilities is attributed to lighting. Medical procedures and routine tasks require high light levels. At the same time, a safe and effective healthcare facility utilizes lighting to promote feelings of well-being, comfort, and safety. The physiological and psychological effect of adequate levels of lighting minimizes stress, reduces errors, and aids in the diagnosis, treatment, and recovery of patients.
Architects translate this understanding into flexible lighting that is adaptable while meeting specific requirements for users’ safety by implementing fundamentals of lighting design elements such as color, illuminance, and direction. (Healthcare: Lighting Design Goals, 2017). The performance, efficiency, and comfort provided by successful lighting design can serve as a measurement of effectiveness. Through the examination of specific healthcare lighting solutions in hospitals as case studies and an analysis of evidence-based design, studies quantify the effects lighting on hospital staff, patients, and their families and guide the discussion towards a successful lighting design. I believe this leads to a need for next generation lighting design that provides flexibility for its users.
Fundamentals of Lighting
I decided to step back and looked at the foundations of lighting design. There are six design parameters, introduced in 1933 by the innovative lighting design firm, L’Observatoire International, used today in the theoretical and practical aspects of lighting: illuminance, luminance, color and temperature, height, direction and distribution, and density (Hervé Descottes, 2013).
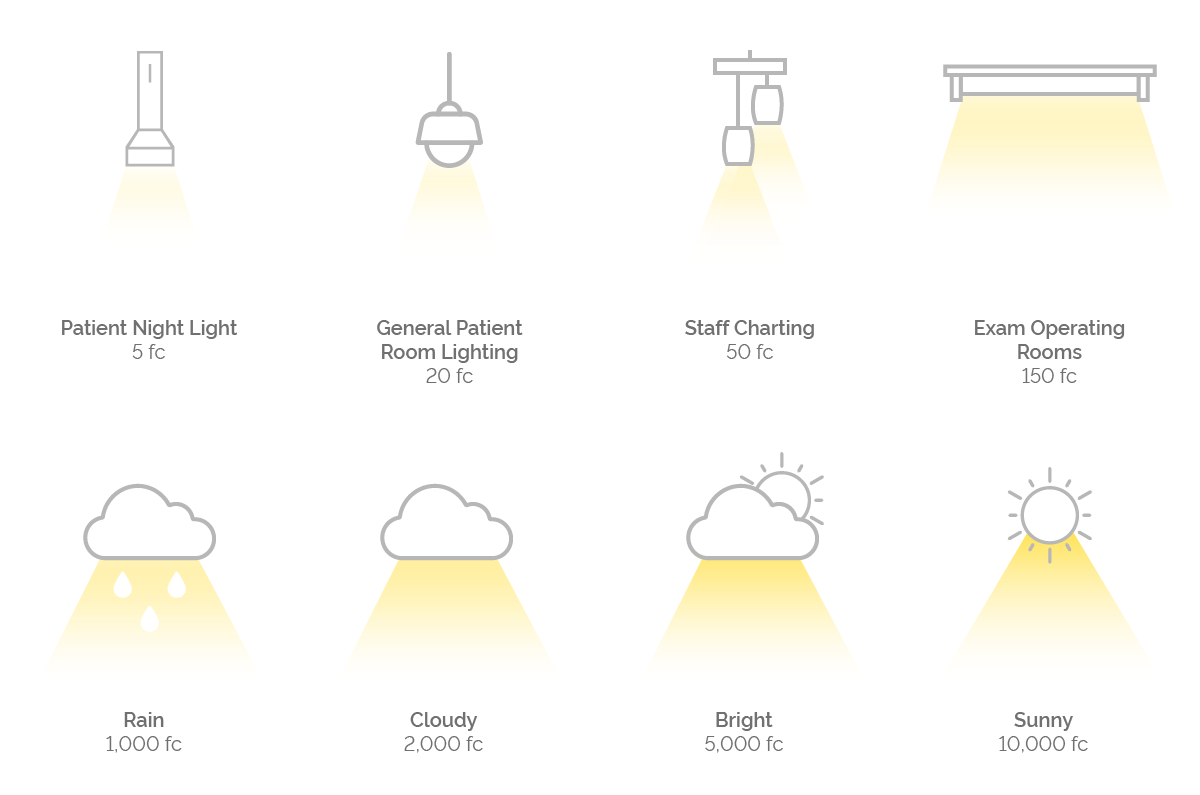
Illuminance is the actual amount of light emitted by a light source that lands on an object or a given surface area. Quantity of light has a direct correlation to human physiology. A study from the University of Toronto Scarborough shows that human emotion, whether positive or negative, is felt more intensely under bright light. The study asked participants to rate a wide range of things such as, the spiciness of chicken-wing sauce, the aggressiveness of a fictional character, how attractive someone was, their feelings about specific words, and the taste of two juices under different lighting conditions. The results found that under bright lights emotions are felt more intensely. Participants wanted spicier chicken wing sauce, thought the fictional character was more aggressive, and felt better about positive words and worse about negative words (Alison Jing Xu, 2014).
Color and temperature of light alter the way we perceive objects and their surroundings. Different temperatures of light generate different physiological effects. Cool white light, simulating daylight, suppresses melatonin and increases serotonin, and is optimal for participating in activities. Warmer light temperatures trigger melatonin, which is the precursor to sleep. It is crucial for lighting temperatures to be properly balanced, so the body will generate dopamine, serotonin, cortisol, and melatonin in the right quantities at the right time of day (Oca, 2017).
Typically, commercial and residential lighting Kelvin temperatures fall somewhere on a scale from 2,000k to 6,500k.
The height of a lighting fixture is one of several variables that affect the intensity, spread, and perceived brightness of a given light source. Put simply, the higher the light source, the greater the surface area illuminated, which can lead to a perception of less privacy. For example, the height of a reading light source in a patient room is typically an arm’s length from the patient. This reinforces control and possession of the space, which serves as a means of reassurance. Family-oriented spaces like waiting rooms may have a suspended architectural fixture over nourishment areas, which allows the light source to be sufficiently removed yet close enough to shower the visitors in a blanket of soft light. The light transition from hospital entrances (public space) to corridors (private spaces) is often a function of height. (Meraj & Islamia, 2017).

Distribution refers to the direction from which the light approaches an object or space, the shape and size of the area the light is covering and the quality of the light (sharp or diffused) (Gillette, 2008). People who work in a typical work environment tend to prefer a mixed ratio of luminaire distribution of direct and indirect light.
Density controls the movement and rhythm of a space through quantity and spatial composition of the light sources. It can be defined by two parameters – the number of fixtures in an area and the organization or grouping of the fixtures.
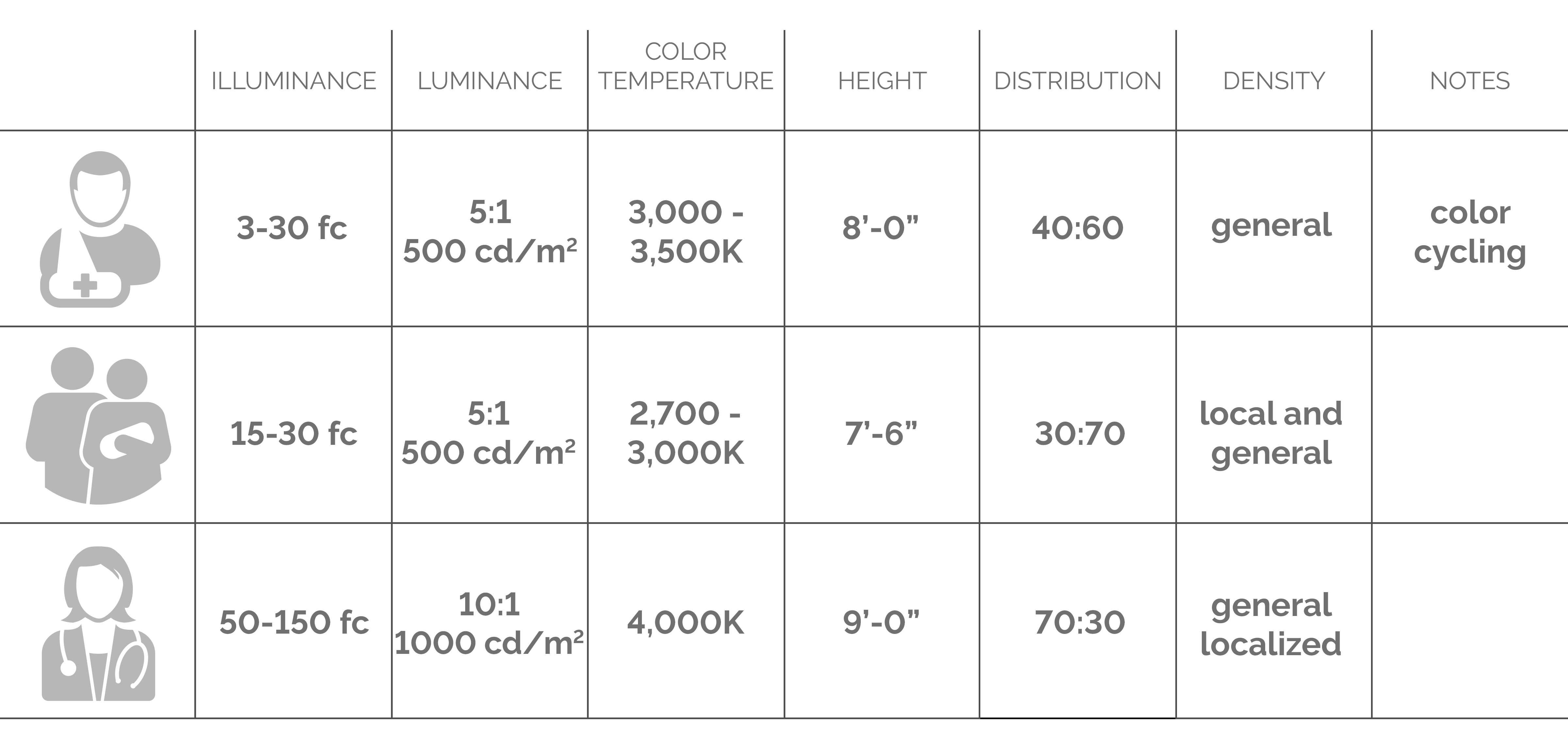
The Users of Healthcare Lighting
There are three distinct user groups in a healthcare setting: patients, families, and staff.
Patients are the most diverse user group in healthcare. Patients range from small infants in the NICU to end-of-life adults with a wide range of outpatient and inpatient care in between. Light can affect alertness, pain, sleep, mood, comfort, experience, and circadian rhythm. It stands to reason that light plays a pretty significant role in the patient environment. Medical inpatients are often exposed to light levels that increase sleep-wake disturbances, negatively affecting mood and pain. However, higher light exposure is also associated with fewer falls while getting in and out of beds.
For patients, the most important aspect of lighting is flexibility. All user groups must share the patient space, so multiple needs must be met, while also promoting the healing process for patients.
Hospitals are naturally stressful environments for family members. At entrances and waiting areas, light plays an important role in creating a welcoming and friendly atmosphere. Lobbies and transition spaces must put the patient and the visitor at ease instantly. Families or visitors, often find themselves perched on window sills, have little or no designed space within the patient room and rarely have access to lighting controls.
Staff members need to perform a range of complex tasks: charting, filling prescriptions, administering medication, and performing other critical patient-care tasks in their work environment. For example, if charting is done in the patient room, the lighting levels are often insufficient, and the staff strain their eyes. So, they will do charting outside the patient room rather than disturb the patient with more light, which can lead to dangerous charting errors.
My Project
Throughout the Healthcare Design Program and my professional career, I have watched thoughtful lighting design be neglected even when a project is said to focus on “patient-centric care”. The lighting needs for hospital user – patients, families, and staff – are often paradoxical, and for my thesis project, I wanted to explore a holistic design in the lighting realm.
Too often in student projects, ideas and design intent never go past computer modeling. I used my extensive background in set design and construction to design and build the largest architectural model of my academic career – a mock-up of a full-size patient’s room (15’ x 20’). I designed a dynamic lighting system for the comfort of each of the distinct user group, altering the illuminance, color temperature, and distribution accordingly. A key feature of this design is its adaptability into potential new door reading technology, which could trigger each lighting scheme based on hospital-issued badges.

I developed lighting presets for each user group informed by evidence-based design. Patient level lighting was the default preset with full controllability of their surroundings. Upon a staff or family member entering, the door reader would trigger staff or visitor lighting preset to transition at a slow gradual rate to avoid abrupt changes in intensity. A light above the sink would flash red to direct users to wash their hands and the light would transition to green over the recommended duration for proper hand washing. As the staff or visitor leaves the patient room, the door reader would trigger the patient preset lighting to slowly transition back.
Within a month, I completed the construction and hosted an open house to have participants provide feedback on the lighting design and automation system. The open house was an opportunity for participants to experience firsthand the proposed lighting design and technology in real time. Participants had an opportunity to ask questions or provide some feedback through questionnaires comparing their past healthcare experiences with the prototype room.

The Results
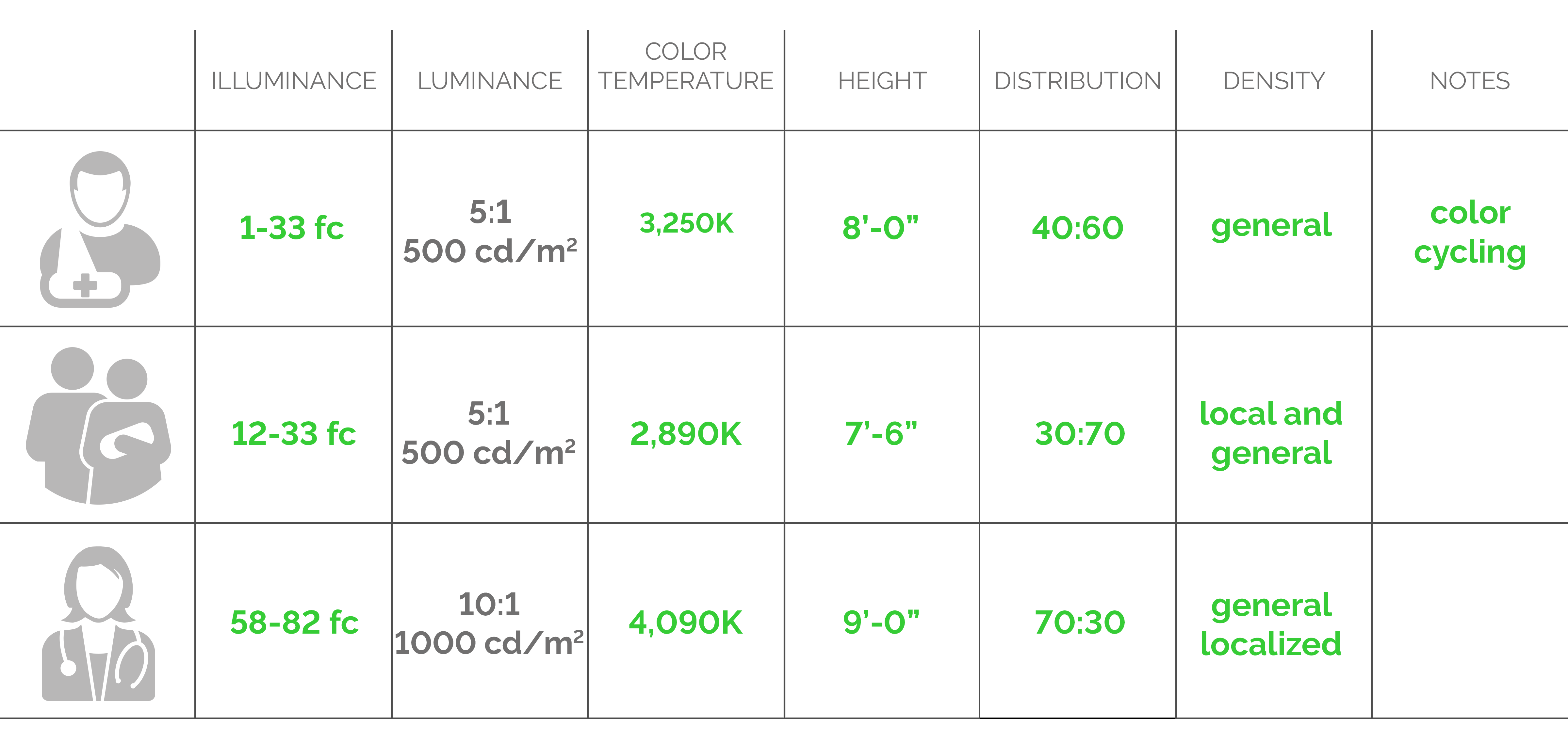
I had numerous participants that covered the diverse range of user groups of patients, visitors, and staff as part of my open house.
In the questionnaire, I aimed to compare current healthcare lighting designs to my proposed lighting design. Many patients and visitors were unsatisfied with the lighting designs they experienced in previous healthcare settings. However, all staff participants felt the lighting designs they experience at work allowed them to effectively do their job. These differing perspectives make sense since most design professionals design lighting to align with the static, standard IES requirement for examination rooms, which is too bright to be comfortable for patients.
100% of participants felt my proposed dynamic lighting design was satisfactory to promote healing and comfort, assimilate elements found at home, and allow the staff to perform their job effectively.
Most of the participants found it important to have control over the lighting around them. Visitors liked having a light indicator over the sink reminding them to wash their hands prior to entering the patient room, and patients recognized and appreciated this detail. Staff members did not have as much reaction to the indicator light, likely because hand-washing is intuitive for them.
Staff level lighting was the most discussed lighting topic. Although many participants felt the light level was pleasant, there were others who felt the staffing light levels were too bright. One participant noted it was “unpleasant, but necessary.”
Final Thoughts
This project affirmed lighting is an integral element of design, especially in a healthcare setting, where it is directly corelated to patient recovery time, visitor comfort, and staff job performance. The design has the potential to set the stage and standard for future generations of lighting design in a healthcare setting and have positive impacts on its very distinct user groups.
I use automatic transitioning lights when designing for theatrical performance. This technology – the ability to shift lighting levels dynamically – is the key. These “smart” LED light fixtures can be integrated into the television, music system, the weather, and time of day. Which shifts the questions to “can we have a fully integrated or “smart” patient room?” to “when will we have a fully integrated or “smart” patient room?”

This project was not only to combine two unique passions of mine, but merge technologies and perceived environments. I will carry the comments from the open house with me as I continue my healthcare design career.
I was able to complete this project with the help and support of a number of special individuals. My parents and other family members who were central in the construction of the room. It was their continual support that pushed me to finish this second master program. Thank you to Tarkett Flooring and Fishman Flooring who graciously donated enough VET flooring for the mock up and provided a quality product to showcase. Many thanks to my advisor, Bill Willoughby, who saw an exceptional project and moved mountains to support me. Lastly, to DesignGroup, for acknowledging the value in continuing education.

Anastasia Markiw, AIA, NCARB, LEED Green Associate // Project Architect
Anastasia offers an innovative perspective to her position as a Project Architect by attending the only post-professional Masters in Health Care Design program in the country. She has advanced her understanding of healthcare architecture through an appreciation for patient care through the use of medical frameworks and design. She strengthened her leadership skills by volunteering in the community and accomplishing the highest Girl Scouts achievement; the Gold Award. Anastasia is fueled by her passion for lighting design, which aids in her understanding of the connection between healing spaces and their intangible experiences; she believes that a working coexistence between architecture and sustainable technology can supply a multitude of design possibilities for a space and its occupants.
Hero Image: © Sami Saunders Studio