Over the generations, patients have noticed drastic changes in their hospital experience. When a patient in the Silent Generation (1925-1945) was admitted to the hospital, they likely stayed in an open ward, segregated by both gender and race. Baby Boomers remember semi-private rooms with three to four patients per room and walking down the hall to shared toilet rooms. They also recollect paying extra if they wanted a room with a TV, something that is unheard of today. The majority of those in Gen X had televisions and telephones at home; therefore, that expectation carried over to their inpatient hospital stay. First, it was one TV and one telephone per room, shared by two patients. Later it was one TV and one telephone per patient. Inpatient rooms began to transition to all-private rooms, but the changes didn’t stop there.

Technology was continuing to advance, and cell phones made their appearance. It is rare to find a Millennial without a cell phone in arm’s reach, and again, this impacted the inpatient room design. With so many patients bringing their own phones, the need for a corded telephone in the patient room has almost disappeared, with some facilities installing a jack, but only bringing in a telephone if requested by the patient. More facilities are installing USB receptacles for patients and families to easily charge their personal devices.
Technology Impact
This ongoing evolution of technology continues to influence the inpatient room today. Throughout history, we have seen the inpatient room and inpatient units steadily increase in size; however, as technology is delivered in smaller and smaller packages, will we begin to see the size of inpatient rooms decrease or will there simply be more technology introduced to fill the void? Generation Z may never experience a semi-private patient room. For them, patient rooms have always had their own toilet room and their own TV. In their thinking, weren’t you, as a patient, expected to bring your own phone?
Meanwhile, tiny technology has made its presence. This wearable technology tracks your activity, heart rate, distance walked, and calories burned. A smart watch gives instant access to messages, email, phone calls, and syncs to your fitness tracker. Tiny technology is making the smart phone look clunky and outdated, yet the smart phone market remains strong. But what if….
Patient Impact
What if, when you are admitted to the hospital, you are given a unique ID number that is also entered into the hospital’s facility infrastructure? You simply download an app, and the doors to improving your inpatient experience are wide open. From the comfort of his hospital bed, Jayden, the Gen Z patient, can quickly order his next meal and learn more about his diagnosis. There’s no need for him to call the nurse to dim the lights, to lower the blinds, or change the temperature in his room. He can do that with a simple slide of his finger on the app.
Just click a screen on the app to change the TV channel or to lower the volume. Although sound-masking has seen limited use in hospitals, individual patient control could improve patient satisfaction, thus raising a hospital’s HCAHPS scores. For assistance, a patient is no longer linked to the unknown voice at the other end of the cord, but instead simply FaceTimes with the nurse on call.

Family Impact
Could this handheld technology bridge the gap of the unknown by bringing information to the patient and family? It may be as simple as notifying a patient that they’ll be taken to testing during a certain timeframe or that the rounding physician is expected in their room in a specific one-hour window, freeing family members to grab a bite to eat and still be present to speak with the doctor.
Generational Impact
With the American population over the age of 65 projected to increase from 14.5% in 2015 to 18.2% in 2025 [ 1 ], the immediate future of healthcare is projected to cater to the Baby Boomers. According to a national study performed by DesignGroup, analyzing the technological capabilities of 164 individuals, a staggering 97.6% boasted above-average technological comfort with an equally impressive 95.7% claiming mobile application-based proficiency [ 2 ]. Of the 42 Baby Boomers responding, 97.6% expressed technological comfort and 92.9% conveyed mobile application-based proficiency. 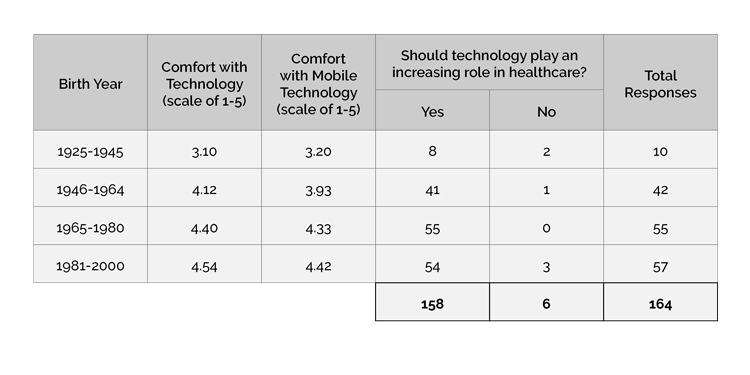
This study highlighted technology’s increasing role in healthcare. In addition, it showed patients’ growing interest in education related to their diagnosis with 97.6% of participants placing importance on the accessibility of this information. Equally important, the study found that 70.1% of the sample population would prefer to communicate with their healthcare provider via text or FaceTime, methods not currently available in hospitals. 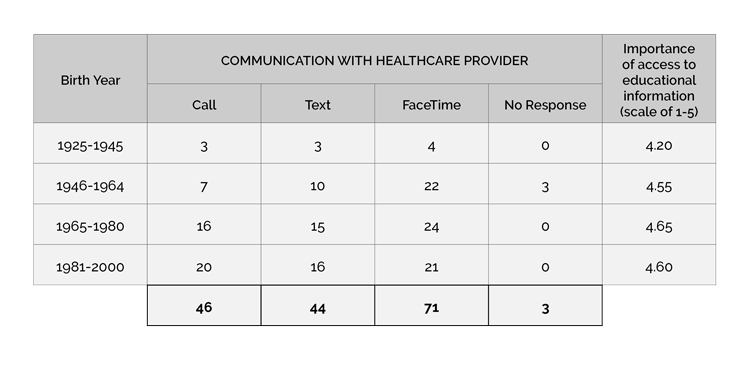
While the benefit of such technology would certainly transcend multiple generations, education would be key to its success, particularly with the aging population. This introduction of patient-controlled technology into inpatient care could be a catalyst for bringing multiple generations together. While the Boomers taught their kids how to tie their shoes and ride their bikes, is it possible that these “kids”, who are now adults, will trade roles and teach the Baby Boomers the ins-and-outs of the inpatient technology world?
Staff Impact
The benefits of technological advancements within the inpatient unit don’t end with the patient. These changes also directly impact the healthcare provider.
The fast-paced nature of our world today has conditioned people to expect everything to happen instantly. If something takes longer than 10-15 seconds, it is a waste of our time and certainly cannot be efficient, or so we think. Imagine this same mentality lying in a patient bed. Will this instant access only exacerbate the demand for clinicians’ time? A patient might text their nurse or physician, but if the care provider doesn’t respond within 30 seconds, are they sending follow-up messages? The ease of access is “good for them [the patient] and I appreciate that fact, but it adds more to my work,” according to a survey respondent who works in the healthcare industry. Will this direct access only feed the monster of instant gratification, demanding more and more from clinical staff?
This onslaught of data and demand for time must be managed, yet still allow the critical communications to flow unhindered, or we will likely see increasing numbers of cases of healthcare provider burnout and a resulting decrease in patient satisfaction. As another survey respondent stated, “They [doctors] no longer get to have the one-on-one time needed to explain because they [doctors] have too much documentation.” In an age where healthcare compensation is directly tied to patient satisfaction and improved overall patient health, capitalizing on a system catered toward increasing quality of care must be balanced with providers’ mental stamina.
If an inpatient app were to give patients more control over their environment and if that app also funneled patient requests to the appropriate staff member, this would free the clinicians to attend to more patient care issues. Meanwhile, other employees must be available to troubleshoot why a patient’s personal device is not properly connecting to their room controls, to re-situate a patient in bed, to support those patients who do not understand or are not in a frame of mind to handle technology, and to assist with other non-clinical requests.
For example, if one nurse on one inpatient unit in one hospital spent an average of 26 minutes per shift answering non-clinical patient calls, how substantial could the time savings be if this one scenario was repeated across every inpatient unit?
Infrastructure Impact
As the use of technology increases, the supporting infrastructure must be modified to handle this change. From additional power to wireless access points, the impact will be significant. Justin Schultz, electrical engineer with Korda Engineering, shared that many commonly think, “If it already has power, why not just connect it to the network?” He explained that the missing link is in these building components having the ability to connect to a network and ultimately be controlled through a common network interface. This must be provided by manufacturers and is driven by the demand of building owners and facility managers. Although the various building control systems (lighting, HVAC, and security) may reside on the same network, they may not currently talk to each other.

In addition to the impact to the building infrastructure, there is a requirement for software to tie these systems together. As software is developed to connect building systems, the same software must also be configured to limit control by outside guests. As facilities investigate the opportunities to allow patients to control the built environment around them, one of the largest questions that arises is how to maintain security – securing the system so patients can only control their specific room, securing the system so patients cannot access other patients’ information, and securing the system from hackers. One survey respondent put it best, “It’s too easy for things to be hacked.”
Despite the costs associated with remotely controlling building systems, the risks associated with relinquishing limited control of these systems to patients, and the personnel costs associated to supporting the ever-increasing technology in patient care, there are myriad benefits that hospitals can reap from these investments.
Final Impact
Patients gain greater control of their own patient experience, raising HCAHPS scores and potentially reimbursements. Families can be more easily involved in their loved one’s care, improving their satisfaction and desire to return to the same hospital. Clinical staff is freed from tedious non-clinical tasks to focus on improving patient care, allowing them to do more of what they love and encouraging them to stay with their current employer. Building systems that talk to one another can be more easily monitored through one platform, allowing the facilities’ staff to catch and correct problems before they become a major cost.
Although the response toward technology in healthcare was positive, multiple respondents to the technology survey expressed strong concerns about losing in-person time with providers, with physician overwork and burnout causing them to leave the profession, and with network security and data breaches. While they see the value that technology can bring, there is still hesitation about the extent to which it should be integrated.
As the impact of technology continues to grow, the human aspect driving healthcare design must remain at the forefront of our thinking. However, Daric Hess, senior principal with Heapy Engineering, summarized it well, “Technology will continue to be the driver for the next generation of patient rooms.”

Alicia Radcliff, NCARB, ACHA, AIA, LEED AP BD+C // Project Architect
Alicia is very passionate about healthcare design. She looks at each new project like a puzzle and loves to find the best possible solutions. She enjoys listening to clients describe their process and finding new ways to create efficiencies. Alicia provides architectural implementation throughout the planning and design process and is involved with projects through construction administration.

Matthew Pierzchala // Project Associate
Matthew’s interest in technologically driven design and adaptive reuse bring a forward-thinking perspective to the world of healthcare design. Believing that architects act as the spokespersons of the built world, Matthew finds that the best architecture often comes from the synthesis of sustainability and innovation. He has used these passions to help shape inspiring and healing spaces in over a dozen medical institutions, from Chicago to Washington DC.
References ↩ 1. Calculated by authors from U.S. Census Bureau, “U.S. Interim Projections by Age, Sex, Race, and Hispanic Origin,” 26 August 2004. ↩ 2. Independent research on technological knowledge and comfort levels with 164 respondents. ↩