When the pandemic struck, hospitals found themselves unprepared, largely because COVID-19 patients disrupted the typical ED model. Amy Nuzum says Observational Units could be a key to managing this crisis long-term.
By: Amy Nuzum, AIA, NCARB // Project Architect, Project Manager
First, the good news: COVID-19 numbers in the United States are stabilizing. Now the not-so-good reality: We’re still far from victory. It’s unlikely a vaccine will be available sooner than the end of 2021, and distributing it on a global scale will be a massive challenge. So the healthcare industry must continue to adapt to the crisis.
One component of a hospital’s success is the Observation Unit (OU). Also known, in the context of this article, as a Clinical Decision Unit (CDUs), OUs are an area where Outpatients can be evaluated over a period, up to 23 hours, separate from the Emergency Department (ED). Ideally located adjacent to ED, OUs provide a place where potential COVID patients can be consulted more safely, with a dedicated group of providers and staff. It’s just one strategy for the long-term reality of managing a pandemic. These units allow physicians to provide more specialized testing to create a more through patient diagnosis which typically require more time than a typical Emergency Department encounter.
At DesignGroup, we’ve studied the need for, and benefits of, OUs. We think they’re a smart strategy for systems that can accommodate it. For some facilities, space constraints make it a challenge to create an OU today — but worthy of consideration in future planning. For others, reconfiguring existing facilities may be possible. We realize it’s not a panacea – it can require changes to staffing and managing a new space and patient flow. But for administrators who plan well — especially those who may have received CARES Act funding for COVID response — it could be a smart investment
Here’s closer look at who, and how, Observation Units can help.
PATIENTS: Safety and Reassurance
An OU can help alleviate fear for the patients and their families. Because no one is permitted to accompany a COVID patient in the hospital, the design of this space can help comfort the patient as they wait for a diagnosis alone. OUs are a quieter, more soothing environment in contrast to the ED. There are softer details: dimmable lighting, reduced ambient noise, and a calmer atmosphere (clinical teams are rarely rushing about), patients experience less stress, a compelling and positive factor in their treatment.
The isolation, of course, serves a purpose: it promotes safety and ease for non-COVID patients. Emergency room visits dropped significantly during the shut-down, as people were less at risk staying in and working from home. As communities gradually open back up, and sports, commutes, and other activities resume, EDs are seeing more of the typical traffic mixed with COVID cases. It’s crucial to keep them apart. Any unit in a hospital utilized to respond to this pandemic must quarantine sick patients in a negative-pressure vacuum to eliminate cross-contamination with non-Coronavirus patients, visitors, and caretakers. CDU’s can be designed to accommodate negative pressure environments, while not occupying the traditional footprint of a critical care unit and can also be a standard room when the need for specialized separation is not required.

OPERATIONS: Cost Savings
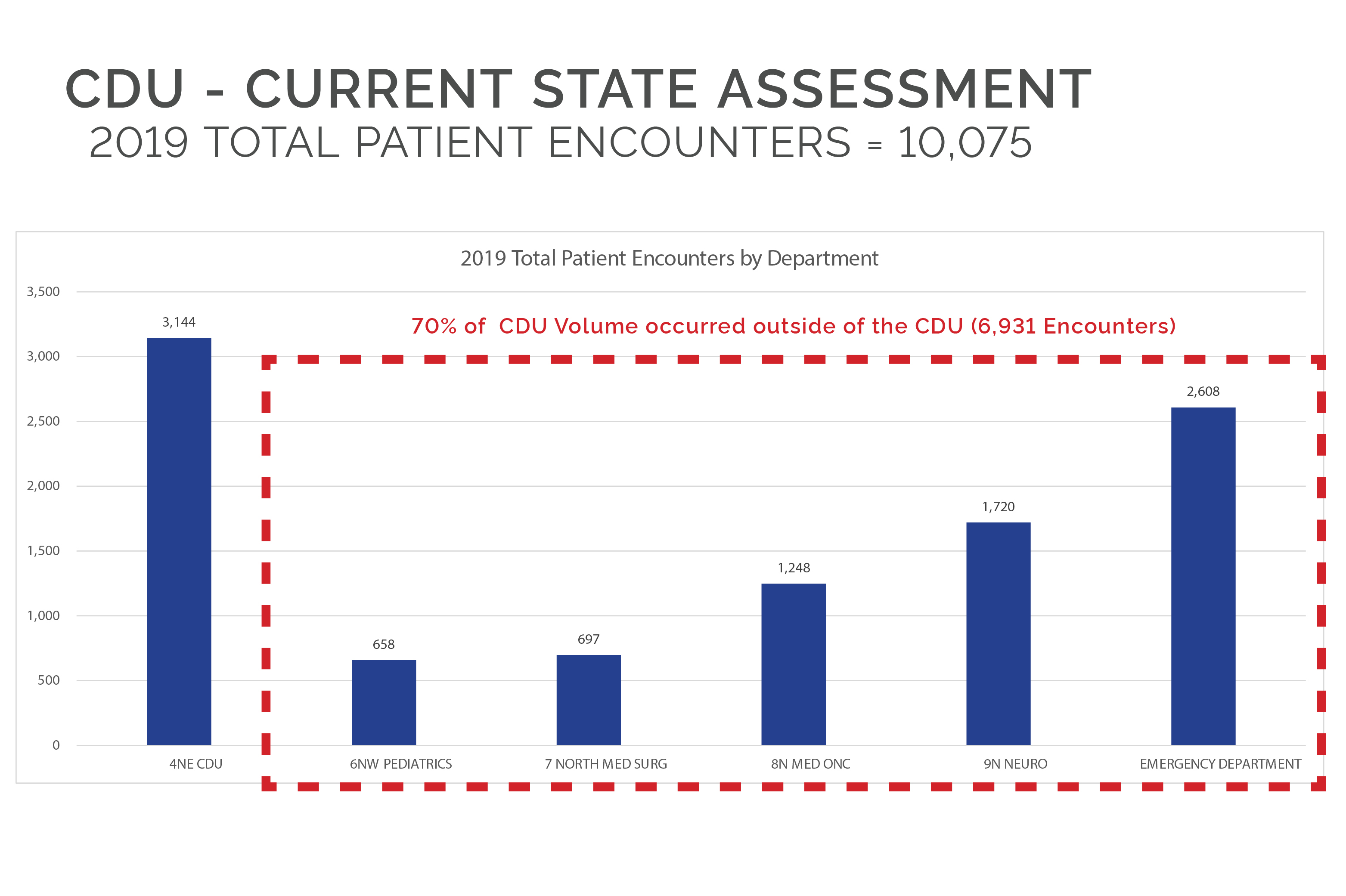
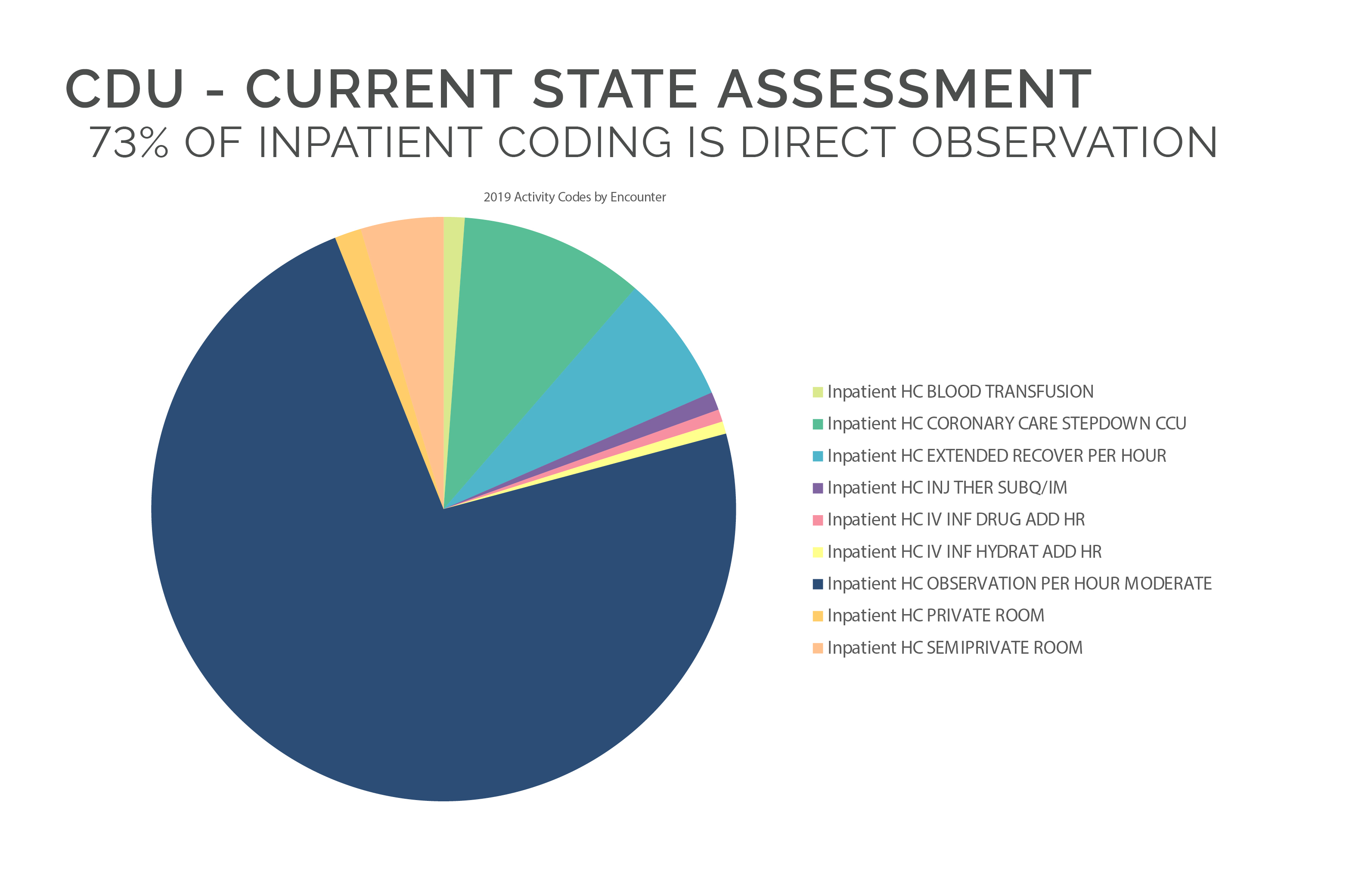
DesignGroup conducted a recent study for a hospital that indicated their volume would support a dedicated OU. Often, the hospital embedded patients in other units – a logistical nightmare that costs the hospital when patients occupy highly valuable space and there are delays in discharge, an avoidable increase to that individual’s length of stay. OUs streamline this kind of temporary inefficiency. And that’s a good thing, because just this month, the Center for Medicare and Medicaid Services (CMS) proposed cuts for reimbursements in 2021 for some of the most lucrative categories and nearly all surgical specialties. If those cuts happen, it only makes sense that hospital volume will need to increase maintain status quo. Recovery space in those departments will become more coveted and there may not be excess inpatient rooms to overflow critically ill patients.
CMS did, however, propose temporary increases tied directly to the current COVID-19 pandemic, as well as waived many restrictions on maximum and minimum lengths of stay during this surge, so perhaps this is the best time to plan for this type of patient and OUs seem to be the best solution. It answers the conundrum: You can’t keep these patients in the ED, but you also don’t want to admit and monopolize an Inpatient Room which may be needed for a patient directly associated with a specific department.
STAFF: Flexibility and Cooperation
Planning these units adjacent to the ED, near the Ambulance Entry, with surrounding resources such as advanced imaging machines, is ideal for managing COVID care. The OU provides overflow, allowing the ED to expand and contract as required. Undeniably this adds complexity to operations (which staff is responsible for the COVID patients?), and requires a cooperative workflow, however, OUs create a better synergy of patient care.
The goal for the ED is to shorten the average length of stay and have the patient admitted or discharged without lingering for hours. The OU allows the hospital to manage more complicated cases and allows the Emergency Department to do what is does best, treat relatively low-acuity patients in a timely manner.
Many doctors have said this coronavirus has forever changed the industry and brought superior safety and humanity back into healthcare systems. The OU provides a buffer of time to curate the most comprehensive plan and execute the best course of action for the patient.

Amy Nuzum, AIA, NCARB // Project Architect, Project Manager
Amy offers a strong perspective in all disciplines and scales of architectural practice. She has a great deal of experience in large master plan studies, most recently with a large downtown Midwest healthcare campus. Amy has also spent many years in retail design, on innovation teams creating new prototypes for branded environments. Translating this focus to the healthcare realm as it relates to the overall patient experience is an exciting challenge for every individual project and client.